
What is chemsex?
Date of current publication: April 25, 2025
Lead authors: Jeremy D. Kidd, MD, MPH; Justin Alves, MSN, FNP-BC, ACRN, AACRN, CARN, CNE; Rohit Mukherjee, MD
Writing group: Susan D. Whitley, MD; Timothy J. Wiegand, MD, FACMT, FAACT, DFASAM; Sharon L. Stancliff, MD; Brianna Norton, DO, MPH; Narelle Ellendon, RN; Christopher J. Hoffmann, MD, MPH, MSc; Charles J. Gonzalez, MD
Committee: Substance Use Guidelines Committee
Date of original publication: April 25, 2025
Chemsex, a term used predominantly among some subsets of men who have sex with men (MSM) and transgender individuals, refers to the use of drugs before or during sex with the intent of enhancing or altering the experience Coronado-Munoz, et al. 2024; Ivey, et al. 2023; Sang, et al. 2021; Evers, et al. 2019; Lawn, et al. 2019; Sewell, et al. 2019. It is a phenomenon in which drug use and sex have a specific interplay, sometimes influenced by co-occurring sexual compulsivity Carrico, et al. 2012; Grov, et al. 2010; Kelly, et al. 2009, and can include various types of sex (e.g., oral sex, anal or vaginal penetrative sex, masturbation, online sex, group sex). Although chemsex is most closely associated with stimulants like methamphetamine (MA), it can involve a variety of substances. Alcohol use before sex is common, but alcohol use alone is generally not considered chemsex.
Individual experiences of chemsex vary, but there is often a shared language and culture (see Table 1, below). The shared language and practices of chemsex and its occurrence in marginalized communities differentiate it from other forms of sexualized drug use. Some individuals find sex partners through geosocial networking apps (e.g., Grindr, Scruff), which have their own chemsex language and symbols (emojis). The prevalence of chemsex behaviors is difficult to estimate; most epidemiologic studies of chemsex rely on samples of treatment-seeking individuals UNAIDS 2024; Harm Reduction International 2021 and likely underestimate prevalence.
| Abbreviation: GHB, gamma hydroxybutyrate. | |
| Table 1: Common Terms Used To Describe Chemsex | |
| Colloquial/Slang Term(s) | Meaning |
| (parTy) favors | Typically methamphetamines or cocaine |
| Bump, booty bump, boof | Use intrarectally or intravaginally |
| G, dose, Gina | GHB, flunitrazepam |
| G-out | Overdose on GHB or pass out |
| Hit | Sniff or smoke (i.e., inhale) |
| Host, travel | Whether or not you are able to go to another location for sex |
| K, special K | Ketamine |
| K-hole | A type of ketamine overdose resulting in a dysphoric dissociative state |
| Overamping | Unpleasant or undesired physical or emotional symptoms from overusing stimulants |
| parTy, PnP, party n play | To use drugs and have sex |
| Poppers | Amyl nitrates or nitrites |
| Rock, hard | Crack cocaine |
| Slam | Use intravenously |
| Swirl | Initial intoxication/high |
| Tina, T | Methamphetamines |
Why do people engage in chemsex?
People may engage in chemsex for a variety of reasons, including to:
- Enhance sexual satisfaction
- Reduce inhibitions or engage in sexual encounters and activities that might feel more intimidating when not under the influence of substances
- Make social connections, especially with other MSM
- Feel sexually desired
- Cope with stigma related to HIV status, sexual orientation, or gender identity; stigma-related victimization; negative body image; loneliness; or social isolation Jaspal 2022; Ahuja, et al. 2021; Bohn, et al. 2020; Hickson 2018; Pollard, et al. 2018
- Offset adverse sexual effects associated with prescribed medications or chronic use of substances such as MA
For individuals engaged in sex work, chemsex participation may be influenced by financial considerations, such as to satisfy a client’s request or enhance or sustain sexual performance (e.g., to increase pain tolerance or facilitate longer sessions).
What substances are commonly used during chemsex?
Although substances used during chemsex differ regionally, MA is the most widely used chemsex drug among MSM and transgender women in the United States and is often used in combination with other substances Rivera, et al. 2021; Nerlander, et al. 2018. Individuals engaging in chemsex often use multiple substances. For example, a stimulant may be paired with a depressant and a hallucinogen, or cocaine may be paired with sildenafil to address cocaine-induced erectile dysfunction. Benzodiazepines or opioids may be used to counteract post–drug use crash or overamping (i.e., unpleasant/undesired physical or emotional symptoms) from stimulant use. Alcohol and GHB may be used to blunt the effects of stimulants and reduce inhibitions. Opioids may also be used to delay ejaculation or orgasm and to help “come down” from the effects of a stimulant. Synthetic peptides may be used to enhance sexual desire, prolong erections, or counteract drug-induced erectile dysfunction.
Drugs commonly used during chemsex include:
- MA (as mentioned above)
- 3,4-Methylenedioxymethamphetamine (MDMA)
- Prostaglandin E1 (PGE1) inhibitors (e.g., sildenafil, tadalafil)
- Ketamine
- Gamma hydroxybutyrate (GHB)
- Gamma butyrolactone (GBL)
- Cocaine
- Alcohol
- Some nitrates or nitrites (“poppers”)
- Some synthetic peptides, including PT-141 and melanotan II, that may be purchased online
See NYSDOH Clinical Guidance: Stimulant Use > Table 1: Characteristics of Commonly Used Stimulants for additional information.
How can I talk to patients about chemsex?
Ask patients frankly and nonjudgmentally about substance use, sexual history, and sexual behaviors. Ask questions that avoid making assumptions and ask for clarification about the meaning of any unfamiliar terms. The goal is to create a space in which all individuals feel comfortable speaking openly about their experiences. See the NYSDOH AI resources GOALS Framework for Sexual History Taking in Primary Care and Clinical Guidance: Stimulant Use > Box 1: Talking With Patients About Substance Use.
To start a conversation about chemsex, clinicians can ask:
- Have you used drugs before or during sex in the last 6 months? If yes, what do you use and how frequently do you use these substances to have sex?
- When was the last time you used drugs or alcohol to make sex more enjoyable? What did you use?
- When was the last time you had sober sex (sex without drugs)? Have you ever had sober sex? Would you like to have sober sex?
For more questions on assessing patients engagement in chemsex, see the Joint United Nations Programme on HIV/AIDS (UNAIDS) Chemsex Toolkit > Service Provider Guide to Addressing Chemsex.
Drawing on principles of motivational interviewing can provide a useful framework for these conversations Miller and Rollnick 2023. When exploring a patient’s reasons for engaging in chemsex, build an alliance by acknowledging and asking about the positive or pleasurable aspects of chemsex, then ask about the less positive aspects of chemsex and explore the patient’s perspective on personal risk and harmful consequences. Some individuals engage in chemsex episodically (e.g., on weekends, at parties) and these may be high-risk episodes. Patterns and methods of use will inform harm reduction counseling (see below).
What is harm reduction?
Harm reduction is an approach that uses practical strategies to reduce the negative consequences associated with substance use and sexual practices. It is founded on respect for the rights of individuals who use drugs (see the National Harm Reduction Coalition). A harm reduction approach promotes positive changes such as reducing substance use and using safely to reduce morbidities, including disease acquisition and transmission, without specifying or promoting abstinence as the only or even ultimate goal. This approach also emphasizes avoiding coercion, discrimination, and bias in the clinical care of people who use drugs. See the NYSDOH AI guideline Substance Use Harm Reduction in Medical Care for information on harm reduction resources, including naloxone, sterile needles and syringes, drug-checking supplies, and drug user health hubs.
Should a patient who engages in chemsex be offered substance use disorder treatment?
Ask the patient whether they are interested in reducing their participation in chemsex or changing patterns of substance use. Although some people who engage in chemsex will meet criteria for a Diagnostic and Statistical Manual of Mental Disorders (DSM-5) substance use disorder (SUD), such as stimulant use disorder, chemsex itself should not be equated with an SUD. After discussing a patient’s chemsex practices, clinicians can use specific tools for assessing the level of substance use and potential presence of an SUD, if indicated.
See the NYSDOH AI guidelines and guidance:
How can I support patients who want to reduce their participation in chemsex?
Maintain a sex-positive approach. Sober sex, rather than no sex, is the goal. This is not to say that patients will never engage in chemsex again. Instead, the goal is being able to have and enjoy sober sex, thereby reducing the frequency of chemsex and its associated health risks. Support patients in making sober social connections, having satisfying sex without the use of substances, and combating internalized stigma and loneliness.
Be familiar with appropriate interventions and referral resources (if needed). Medications, contingency management, and other behavioral health interventions may be helpful for some patients. A multipronged approach that addresses the component needs of the individual is best. However, not all clinicians or facilities are equipped to provide the various treatments or services an individual needs. Prepare patients for the possibility they may be referred to different care providers and services who will coordinate to address different aspects of their care.
For patients who continue participating in chemsex, harm reduction counseling is an essential intervention.
How can I effectively and nonjudgmentally counsel patients on risk reduction?
Chemsex involves drug- and sex-related risks, which vary from individual to individual. First, ask patients about any steps they are already taking to reduce risks associated with chemsex and offer positive reinforcement.
When discussing the health risks associated with chemsex, refrain from judgment and focus on harm reduction strategies. For example, “I’m here to help you continue having fun sexually (chemsex or not) but with fewer risks and harms.”
What are the sexual risks associated with chemsex?
Sexual risks include transmission of or infection with HIV, hepatitis C virus (HCV), and other sexually transmitted infections (STIs), including (but not limited to) gonorrhea, syphilis, and chlamydia Siddiq, et al. 2023; Amundsen, et al. 2022; Moradi, et al. 2022; Guerras, et al. 2021; Blomquist, et al. 2020; Stevens, et al. 2020; O'Halloran, et al. 2019; Sewell, et al. 2018. In 2022, 67% of incident HIV infections were among MSM CDC 2024, and in a study that enrolled participants from October 2017 to June 2018, 1 in 3 infections was among MSM who use meth Grov, et al. 2020. Among MSM, MA use is associated with twice the risk of HIV infection and transmission Colfax, et al. 2010; Ostrow, et al. 2009; Buchacz, et al. 2005. Inconsistent condom use; condomless sex with multiple partners; and anal, rectal, and penile trauma (from longer or intense sexual encounters) increase the risk of HIV and STI transmission UNAIDS 2024.
Topics for patient counseling are outlined in Box 1, below.
| Box 1: Counseling Patients About Potential Sexual Risks Associated With Chemsex |
|
When counseling patients:
|
What are the drug-related risks associated with chemsex?
The risks and relevant harm reduction counseling depend on which substance(s) an individual is using and how they are using them (e.g., injection, inhalation, insufflation, intrarectal, or intravaginal). For example, snorting drugs may cause ulcers in the nasal cavity or a deviated septum, inhalation can damage lungs or lead to barotrauma, injecting drugs may cause skin or soft tissue infections, and intrarectal or intravaginal use can lead to abscesses. Rectal or vaginal use can also cause abrasions and lead to increased risk of acquiring or transmitting HIV and other STIs.
Some individuals take drugs provided to them by other people and may not know exactly what they are using. Additionally, because of intoxication or transient loss of consciousness, individuals may not remember what they have taken. Drug adulteration is also common. For example, the MA supply in the United States is increasingly contaminated with the high-potency opioid fentanyl or other agents such as xylazine Wagner, et al. 2023. Although alcohol consumption alone is not generally considered chemsex, use of alcohol along with other substances (e.g., benzodiazepines, opioids) is associated with higher rates of oversedation, overdose, and participation in other high-risk behaviors Kleinman and Weiss 2022; Tori, et al. 2020; Brown, et al. 2016; Johnson, et al. 2016.
A priority for harm reduction counseling is to help patients develop strategies to prevent drug overdose, overamping (i.e., overuse of stimulants leading to unpleasant/undesired physical or emotional symptoms), and alcohol poisoning; see Table 2, below.
| Abbreviation: GHB, gamma hydroxybutyrate. | |
| Table 2: Strategies for Preventing Overdose During Chemsex | |
| Risk | Strategies |
| Opioid overdose | Counsel patients to:
Clinicians can:
|
| Overamping (stimulants) | Counsel patients to:
Clinicians can:
|
| GHB overdose | Counsel patients to:
|
| Ketamine overdose | Counsel patients to:
|
| Alcohol poisoning | Counsel patients to:
Clinicians can:
|
To address other drug-related risks, clinicians can:
- Encourage noninjection methods of use, educate about syringe services, or prescribe clean syringes; encourage use of personal rather than shared drug-use equipment; provide resources, if available, for community organizations that provide such materials. See NYSDOH AI guideline Substance Use Harm Reduction in Medical Care > Box 1: Harm Reduction Resources in New York State.
- Educate about strategies for safer smoking (e.g., using lip balm) and snorting (e.g., using personal snorting equipment or clean paper instead of dollar bills) to reduce infection risk.
- Educate patients on drug dependence and withdrawal and how to recognize the symptoms: cocaine, MA, GHB/ GBL, and alcohol have a higher risk of dependence and withdrawal symptoms and may require medical treatment; ketamine, MDMA, amyl nitrates, and PGE1 inhibitors have a lower risk.
- Advise on potential drug-drug interactions and effects, such as the risk of:
- Hypotension when using amyl nitrates with PGE1 inhibitors
- Oversedation when using GHB with alcohol
- Hypotension and vomiting when using GHB or alcohol with spironolactone
- Thrombosis when using cocaine or MA with estrogen
- Overamping when using ketamine, cocaine, MA, or GHB with boosted protease inhibitors for HIV treatment or with nirmatrelvir/ritonavir (Paxlovid) for COVID-19 treatment
- Priapism with PGE1 inhibitors
- Syncope/hypotension (e.g., PGE1 inhibitors can cause syncope/hypotension when used with some cardiac medications Kloner, et al. 2018)
- Review the patient’s medications (prescribed, over-the-counter, and supplements) and advise on interactions between these and drugs used during chemsex.
- Recommend and refer for regular oral health care and preventive screening; use of stimulants is associated with dental caries, teeth loss, gum disease, gingivitis, and aphthous ulcers.
- See NYSDOH AI Clinical Guidance: Stimulant Use > Commonly Used Stimulants: Characteristics and Adverse Effects.
Which mental health conditions should be considered in patients participating in chemsex?
Chemsex has been associated with negative mental health outcomes, including paranoid ideation, hallucinations, anxiety, depression, social isolation, psychosis, memory loss, personality change, and suicidal ideation UNAIDS 2024.
Substance-induced psychosis: Episodic and chronic use of stimulants can lead to substance-induced psychosis. Individuals with substance-induced psychosis may experience paranoia, delusions, hearing voices, and tactile disturbances (e.g., feeling of bugs crawling on the skin). Individuals may present to emergency departments with substance-induced psychosis, which can lead to involuntary admission for psychiatric care. Substance-induced psychosis should not be equated with schizophrenia or schizoaffective disorder. Substance-induced psychosis can be episodic and self-limited or recurrent and persistent. If stimulants are used over a long period, related psychosis may become a chronic condition. Compared with other stimulants, MA use carries the highest risk of associated psychosis SAMHSA 1999. When patients present with psychosis validate their emotional experiences (e.g., fear) without directly validating delusional thinking (e.g., paranoia) or perceptual disturbances (auditory or visual hallucinations). It is equally important to ensure that the appropriate treatment is provided or recommended, such as referring patients to and encouraging them to see psychiatrists and other mental health clinicians. The New York State Office of Mental Health offers a directory of mental health programs. In some cases, clinicians can consider prescribing short-term, as-needed benzodiazepines and antipsychotic medications, which may reduce distress and symptoms of psychosis Coffin, et al. 2024; Searles Quick, et al. 2021; Patel, et al. 2019; Wilson, et al. 2012; SAMHSA 1999.
Co-occurring psychiatric conditions: It is important to screen for and treat any co-occurring psychiatric conditions (e.g., depression, schizophrenia, bipolar disorder, attention-deficit/hyperactivity disorder, borderline personality disorder, eating disorders) in patients engaging in chemsex. Treating these conditions can reduce emotional dysregulation and impulsivity overall and improve decision-making in the context of sexual and substance use–related risks. Conversely, drugs used during chemsex can worsen co-occurring psychiatric conditions. For example, stimulant withdrawal can exacerbate co-occurring major depressive disorder (MDD) or cause depression, and even suicidality, in individuals without preexisting MDD.
Should I address consent and safety issues with patients participating in chemsex?
Although individuals who engage in chemsex are often stereotyped as perpetrators of violence and sexual assault, research suggests they are more likely to be victims of these crimes Kramer, et al. 2012. Delineations between kink and abuse and between boundaries and consent can blur in the context of chemsex. Individual experiences and beliefs around these topics vary. Maintain a neutral, nonjudgmental approach when discussing these subjects with patients. Encourage patients to reflect on their personal boundaries, what they are comfortable with, and how they will assert themselves in various situations before they engage in chemsex. For individuals who have experienced physical or sexual trauma, it can be helpful to provide resources for community supports and referrals for trauma-specific care.
Resources
| RESOURCES |
Clinical Consultation
Online Resources
|
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
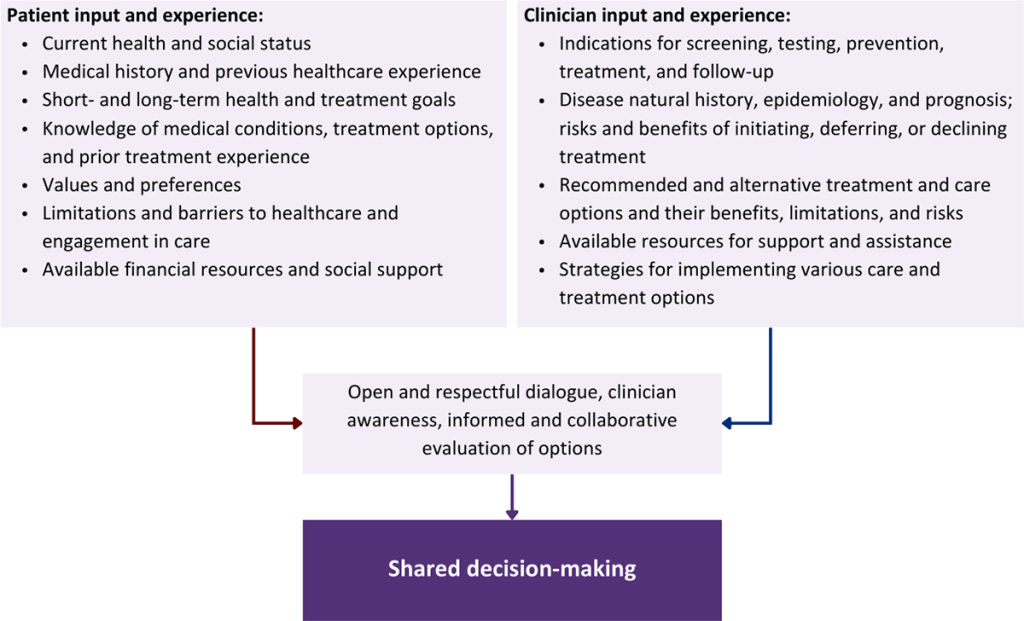
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Ahuja N., Schmidt M., Dillon P. J., et al. Online narratives of methamphetamine use and risky sexual behavior: can shame-free guilt aid in recovery?. Arch Sex Behav 2021;50(1):323-32. [PMID: 32671499]
Amundsen E., Haugstvedt A., Skogen V., et al. Health characteristics associated with chemsex among men who have sex with men: results from a cross-sectional clinic survey in Norway. PLoS One 2022;17(10):e0275618. [PMID: 36197878]
Blomquist P. B., Mohammed H., Mikhail A., et al. Characteristics and sexual health service use of MSM engaging in chemsex: results from a large online survey in England. Sex Transm Infect 2020;96(8):590-95. [PMID: 32139497]
Bohn A., Sander D., Kohler T., et al. Chemsex and mental health of men who have sex with men in Germany. Front Psychiatry 2020;11:542301. [PMID: 33329083]
Brown J. L., Gause N. K., Northern N. The association between alcohol and sexual risk behaviors among college students: a review. Curr Addict Rep 2016;3(4):349-55. [PMID: 27896039]
Buchacz K., McFarland W., Kellogg T. A., et al. Amphetamine use is associated with increased HIV incidence among men who have sex with men in San Francisco. AIDS 2005;19(13):1423-24. [PMID: 16103774]
Carrico A. W., Pollack L. M., Stall R. D., et al. Psychological processes and stimulant use among men who have sex with men. Drug Alcohol Depend 2012;123(1-3):79-83. [PMID: 22088656]
CDC. HIV surveillance supplemental report: estimated HIV incidence and prevalence in the United State, 2018-2022. 2024 May 21. https://stacks.cdc.gov/view/cdc/156513 [accessed 2024 Oct 18]
Ciccarone D., Shoptaw S. Understanding stimulant use and use disorders in a new era. Med Clin North Am 2022;106(1):81-97. [PMID: 34823736]
Coffin P. O., Chang Y. G., McDaniel M., et al. Evaluation of methamphetamine assist packs: as-needed antipsychotics for self-management of methamphetamine-associated psychiatric toxicity. Int J Drug Policy 2024;129:104480. [PMID: 38861841]
Colfax G., Santos G. M., Chu P., et al. Amphetamine-group substances and HIV. Lancet 2010;376(9739):458-74. [PMID: 20650520]
Coronado-Munoz M., Garcia-Cabrera E., Quintero-Florez A., et al. Sexualized drug use and chemsex among men who have sex with men in Europe: a systematic review and meta-analysis. J Clin Med 2024;13(6):1812. [PMID: 38542036]
Evers Y. J., Van Liere Gafs, Hoebe Cjpa, et al. Chemsex among men who have sex with men living outside major cities and associations with sexually transmitted infections: a cross-sectional study in the Netherlands. PLoS One 2019;14(5):e0216732. [PMID: 31086390]
Grov C., Parsons J. T., Bimbi D. S. Sexual compulsivity and sexual risk in gay and bisexual men. Arch Sex Behav 2010;39(4):940-49. [PMID: 19308715]
Grov C., Westmoreland D., Morrison C., et al. The crisis we are not talking about: one-in-three annual HIV seroconversions among sexual and gender minorities were persistent methamphetamine users. J Acquir Immune Defic Syndr 2020;85(3):272-79. [PMID: 32740370]
Guerras J. M., Hoyos Miller J., Agusti C., et al. Association of sexualized drug use patterns with HIV/STI transmission risk in an internet sample of men who have sex with men from seven european countries. Arch Sex Behav 2021;50(2):461-77. [PMID: 32875382]
Harding R. W., Wagner K. T., Fiuty P., et al. "It's called overamping": experiences of overdose among people who use methamphetamine. Harm Reduct J 2022;19(1):4. [PMID: 35034643]
Harm Reduction International. Chemsex and harm reduction for gay men and other men who have sex with men. 2021 July. https://hri.global/wp-content/uploads/2022/10/HRI_Briefing_Chemsex_July_2021_Final-1.pdf [accessed 2025 Feb 18]
Heinala P., Alho H., Kiianmaa K., et al. Targeted use of naltrexone without prior detoxification in the treatment of alcohol dependence: a factorial double-blind, placebo-controlled trial. J Clin Psychopharmacol 2001;21(3):287-92. [PMID: 11386491]
Hickson F. Chemsex as edgework: towards a sociological understanding. Sex Health 2018;15(2):102-7. [PMID: 29321096]
Ivey K., Bernstein K. T., Kirkcaldy R. D., et al. Chemsex drug use among a national sample of sexually active men who have sex with men, - American Men's Internet Survey, 2017-2020. Subst Use Misuse 2023;58(5):728-34. [PMID: 36872623]
Jaspal R. Chemsex, identity and sexual health among gay and bisexual men. Int J Environ Res Public Health 2022;19(19):12124. [PMID: 36231424]
Johnson P. S., Sweeney M. M., Herrmann E. S., et al. Alcohol increases delay and probability discounting of condom-protected sex: a novel vector for alcohol-related HIV transmission. Alcohol Clin Exp Res 2016;40(6):1339-50. [PMID: 27129419]
Kelly B. C., Bimbi D. S., Nanin J. E., et al. Sexual compulsivity and sexual behaviors among gay and bisexual men and lesbian and bisexual women. J Sex Res 2009;46(4):301-8. [PMID: 19148829]
Kleinman R. A., Weiss R. D. Benzodiazepine-involved overdose deaths in the USA: 2000-2019. J Gen Intern Med 2022;37(8):2103-9. [PMID: 35415793]
Kloner R. A., Goggin P., Goldstein I., et al. A new perspective on the nitrate-phosphodiesterase type 5 inhibitor interaction. J Cardiovasc Pharmacol Ther 2018;23(5):375-86. [PMID: 29739235]
Kramer T. L., Borders T. F., Tripathi S., et al. Physical victimization of rural methamphetamine and cocaine users. Violence Vict 2012;27(1):109-24. [PMID: 22455188]
Lawn W., Aldridge A., Xia R., et al. Substance-linked sex in heterosexual, homosexual, and bisexual men and women: an online, cross-sectional "Global Drug Survey" report. J Sex Med 2019;16(5):721-32. [PMID: 30952548]
Miller W. R., Rollnick S. Motivational interviewing: helping people change and grow. Applications of Motivational Interviewing; 2023. https://www.routledge.com/Motivational-Interviewing-Fourth-Edition-Helping-People-Change-and-Grow/Miller/p/book/9781462552795
Moradi S., Moradi Y., Rahmani K., et al. The association between methamphetamine use and number of sexual partners in men who have sex with men: a systematic review and meta-analysis. Subst Abuse Treat Prev Policy 2022;17(1):27. [PMID: 35397571]
Nerlander L. M. C., Hoots B. E., Bradley H., et al. HIV infection among MSM who inject methamphetamine in 8 US cities. Drug Alcohol Depend 2018;190:216-23. [PMID: 30055426]
O'Halloran C., Rice B., White E., et al. Chemsex is not a barrier to self-reported daily PrEP adherence among PROUD study participants. Int J Drug Policy 2019;74:246-54. [PMID: 31739177]
Ostrow D. G., Plankey M. W., Cox C., et al. Specific sex drug combinations contribute to the majority of recent HIV seroconversions among MSM in the MACS. J Acquir Immune Defic Syndr 2009;51(3):349-55. [PMID: 19387357]
Patel J., Frankel S., Tampi R. R. Evidence for using PRN pharmacotherapy to treat undifferentiated acute agitation or aggression. Ann Clin Psychiatry 2019;31(1):54-69. [PMID: 30699218]
Pollard A., Nadarzynski T., Llewellyn C. Syndemics of stigma, minority-stress, maladaptive coping, risk environments and littoral spaces among men who have sex with men using chemsex. Cult Health Sex 2018;20(4):411-27. [PMID: 28741417]
Rivera A. V., Harriman G., Carrillo S. A., et al. Trends in methamphetamine use among men who have sex with men in New York City, 2004-2017. AIDS Behav 2021;25(4):1210-18. [PMID: 33185774]
SAMHSA. Treatment for stimulant use disorders: updated 2021. SAMHSA/CSAT Treatment Improvement Protocols; 1999. https://www.ncbi.nlm.nih.gov/pubmed/35041354
Sang J. M., Cui Z., Sereda P., et al. Longitudinal event-level sexual risk and substance use among gay, bisexual, and other men who have sex with men. Int J Environ Res Public Health 2021;18(6):3183. [PMID: 33808675]
Santos G. M., Ikeda J., Coffin P., et al. Targeted oral naltrexone for mild to moderate alcohol use disorder among sexual and gender minority men: a randomized trial. Am J Psychiatry 2022;179(12):915-26. [PMID: 36285404]
Searles Quick V. B., Herbst E. D., Kalapatapu R. K. Which emergent medication should I give next? Repeated use of emergent medications to treat acute agitation. Front Psychiatry 2021;12:750686. [PMID: 34950067]
Sewell J., Cambiano V., Miltz A., et al. Changes in recreational drug use, drug use associated with chemsex, and HIV-related behaviours, among HIV-negative men who have sex with men in London and Brighton, 2013-2016. Sex Transm Infect 2018;94(7):494-501. [PMID: 29700052]
Sewell J., Cambiano V., Speakman A., et al. Changes in chemsex and sexual behaviour over time, among a cohort of MSM in London and Brighton: findings from the AURAH2 study. Int J Drug Policy 2019;68:54-61. [PMID: 30999243]
Siddiq M., O'Flanagan H., Richardson D., et al. Factors associated with sexually transmitted shigella in men who have sex with men: a systematic review. Sex Transm Infect 2023;99(1):58-63. [PMID: 36283806]
Stevens O., Moncrieff M., Gafos M. Chemsex-related drug use and its association with health outcomes in men who have sex with men: a cross-sectional analysis of Antidote clinic service data. Sex Transm Infect 2020;96(2):124-30. [PMID: 31171592]
Tori M. E., Larochelle M. R., Naimi T. S. Alcohol or benzodiazepine co-involvement with opioid overdose deaths in the United States, 1999-2017. JAMA Netw Open 2020;3(4):e202361. [PMID: 32271389]
UNAIDS. Chemsex toolkit: for clinical service providers in the Asia-Pacific region. 2024 Oct 28. https://unaids-ap.org/wp-content/uploads/2024/11/chemsex-toolkit-for-clinical-service-providers-in-the-asia-pacific-region_05112024.pdf [accessed 2025 Feb 18]
Wagner K. D., Fiuty P., Page K., et al. Prevalence of fentanyl in methamphetamine and cocaine samples collected by community-based drug checking services. Drug Alcohol Depend 2023;252:110985. [PMID: 37826988]
Wilson M. P., Pepper D., Currier G. W., et al. The psychopharmacology of agitation: consensus statement of the American Association for Emergency Psychiatry project Beta Psychopharmacology Workgroup. West J Emerg Med 2012;13(1):26-34. [PMID: 22461918]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | April 25, 2025 |
| Intended users | Primary care clinicians and care providers in other adult outpatient care settings |
| Lead author(s) |
Jeremy D. Kidd, MD, MPH; Justin Alves, MSN, FNP-BC, ACRN, AACRN, CARN, CNE; Rohit Mukherjee, MD1 1Department of Psychiatry, Columbia University |
| Writing group |
Susan D. Whitley, MD; Timothy J. Wiegand, MD, FACMT, FAACT, DFASAM; Sharon L. Stancliff, MD; Brianna Norton, DO, MPH; Narelle Ellendon, RN; Christopher J. Hoffmann, MD, MPH, MSc; Charles J. Gonzalez, MD |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
Guidelines
Guidances
Podcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on March 19, 2026