
Purpose of This Guideline
Date of current publication: May 30, 2024
Lead authors: Jennifer McNeely, MD, MS; Leah K. Hamilton, PhD; Susan D. Whitley, MD
Writing group: Timothy J. Wiegand, MD, FACMT, FAACT, DFASAM; Sharon L. Stancliff, MD; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD; Christopher J. Hoffmann, MD, MPH, MSc, FACP
Committee: Substance Use Guidelines Committee
Date of original publication: October 21, 2020
This guideline on screening and risk assessment for substance use in adults (≥18 years old) was developed by the New York State Department of Health AIDS Institute (NYSDOH AI) for use by primary care clinicians and in other adult outpatient care settings in New York State to achieve the following goals:
- Increase the identification of unhealthy substance use among New York State residents and increase access to evidence-based interventions for appropriate patients. “Unhealthy substance use” refers to a spectrum of use that increases the risk of health consequences and ranges from hazardous or risky patterns of use to severe substance use disorder (SUD).
- Increase the number of clinicians in New York State who perform substance use screening and risk assessment as an integral part of primary care.
- Provide clinicians with guidance on selecting validated substance use screening and risk assessment tools and on providing or referring for evidence-based interventions.
- Promote a harm reduction approach to the identification and treatment of substance use and SUDs, which involves practical strategies and ideas aimed at reducing the negative consequences associated with substance use.
Rationale: In the United States, the use of tobacco, alcohol, and drugs (illicitly manufactured and nonmedical prescription) are among the top 10 leading causes of preventable death, accounting for more than 500,000 deaths per year White, et al. 2020; GBD 2018. Alcohol-related deaths have doubled in the past 2 decades; in 2019, there were more than 140,000 alcohol-related deaths in the United States CDC 2022. Surging rates of drug overdose deaths (often opioid-related) are a public health crisis across the country. In the United States, drug overdose contributed to 1 in 22 deaths in 2021, and there were more than 100,000 drug overdose deaths in the 12 months ending August 2023 CDC 2024; Gomes, et al. 2023.
Patient visits to healthcare settings are an opportunity for clinicians to identify substance use and related problems, offer timely interventions, and provide or link patients to treatment when indicated. Screening and treatment for tobacco use have been widely adopted as core clinical quality measures for primary care CMS 2013, but alcohol and drug use screening is not as widely performed, and use is substantially under-recognized Hallgren, et al. 2020; WHO 2016; Venkatesh and Davis 2000. Screening for alcohol use has been a recommended practice in adult primary care since 1996 Curry, et al. 2018. In a study of 13 states and the District of Columbia in 2017, 81.4% of patients reported being asked about any alcohol use by a healthcare professional; however, only 37.8% reported being asked about binge drinking behavior McKnight-Eily, et al. 2020.
Screening for substance use in primary care is generally well accepted by patients as a marker of quality care Simonetti, et al. 2015; Miller, et al. 2006. However, thoughtful implementation, with sensitivity to stigma and privacy concerns, is essential for patients and clinicians to be comfortable Bradley, et al. 2020; McNeely, et al. 2018.
Substance Use Screening and Risk Assessment: Goals and Definitions
The goals of screening for and assessing substance use risk in primary care vary by practice setting and resources and may include:
- Informing medical care: Substance use is an important aspect of medical history because it can significantly affect disease processes, response to treatment, and exposure to health risks. Knowledge of a patient’s substance use informs a clinician’s diagnosis of other medical and psychiatric conditions and alerts them to associated health risks (e.g., overdose, liver disease) and common comorbid conditions (e.g., depression). Similar to knowledge about a patient’s past medical history, family history, or social determinants of health, knowledge about a patient’s substance use helps clinicians formulate effective patient-centered treatment plans.
- Identifying the need for intervention: A second goal is to identify patients who would benefit from interventions to limit harms related to use and/or reduce their consumption (see guideline section Patient Engagement and Interventions) or patients for whom treatment may be appropriate (see guideline section Diagnosis of Substance Use Disorder). Evidence-based interventions are available, including brief interventions for moderate-risk alcohol use, pharmacotherapy for opioid and alcohol use disorders, and treatment for smoking cessation Patnode, et al. 2021; Patnode, et al. 2020; USPSTF(c) 2020; Curry, et al. 2018; Jonas, et al. 2014; Mattick, et al. 2014. Such treatments can be delivered effectively in a primary care setting, but they remain underused.
- Engaging patients: Another goal is opening the conversation and engaging patients in discussion about substance use. If approached sensitively, a nonjudgmental discussion of a patient’s substance use may reduce perceived stigma, improve the clinical relationship, and facilitate behavior change. Initiating such a discussion communicates to patients that substance use is a health issue that the clinician is concerned about and can offer help for.
Definitions of the terms used throughout this guideline are detailed below.
- Unhealthy substance use: Unhealthy substance use refers to a spectrum of use that increases the risk of health consequences and ranges from hazardous or risky patterns of use to severe substance use disorder. As defined in this guideline, unhealthy alcohol use is use that exceeds U.S. Department of Health and Human Services and Department of Agriculture 2015-2020 Dietary Guideline For illicitly manufactured drugs, less information is available about dosage and health risks of specific substances and preparations, and any use is considered potentially unhealthy. For prescription medications with potential for misuse, any nonmedical use (use of prescribed medication at increased dose or frequency or for reasons other than prescribed) or use of medications that were not prescribed is considered unhealthy.
- Screening: Screening entails asking patients brief questions (or a single question) about substance use and can quickly identify patients with potentially unhealthy substance use. Many of these patients will not have substance use-related clinical signs or symptoms Saitz(b), et al. 2014; Gordon, et al. 2013.
- Risk assessment: Risk assessment entails asking patients additional questions on the extent, duration, and pattern of substance use to determine the clinical significance and severity of use. Assessment tools determine the level of risk (i.e., low, moderate, or high) and thus the potential for negative consequences; see Box 1, below. As shown in Figure 1: Substance Use Screening, Risk Assessment, Diagnosis, and Interventions, risk level and other individual patient factors guide clinicians in recommending appropriate interventions and informing patients about the potential consequences of their substance use McNeely(a), et al. 2016; Saitz 2005.
| Box 1: Substance Use Levels of Risk [a] |
|
|
Note:
|
Screening
| RECOMMENDATIONS |
Screening
|
Figure 1: Substance Use Screening, Risk Assessment, Diagnosis, and Interventions
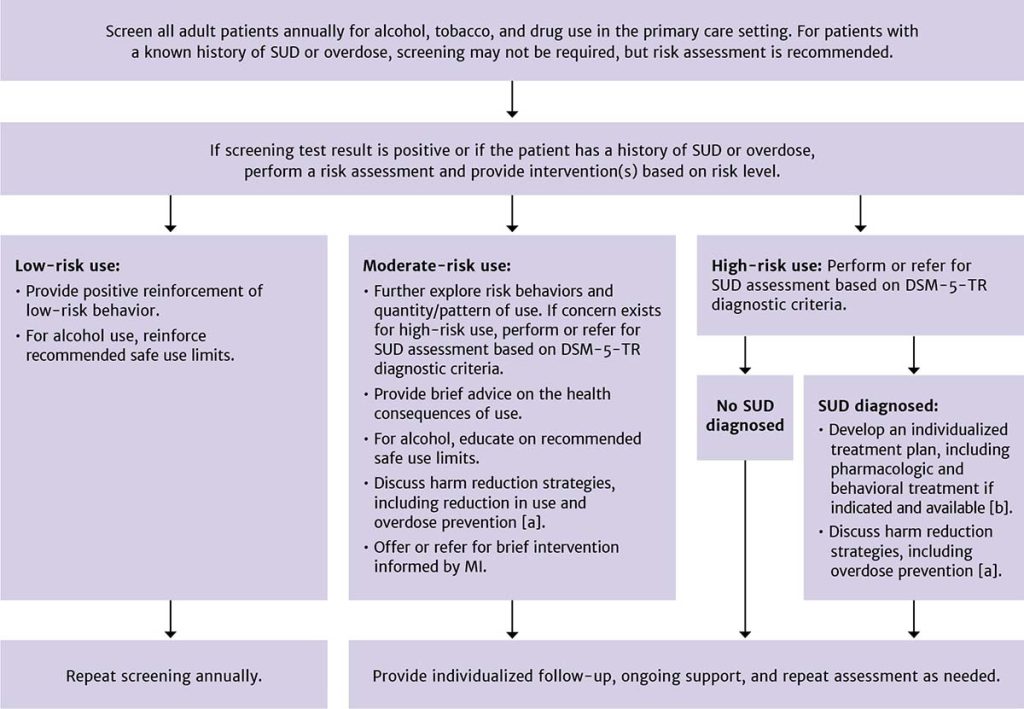
Abbreviations: DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; MI, motivational interviewing; SUD, substance use disorder.
Notes:
- See NYSDOH AI guideline Substance Use Harm Reduction in Medical Care.
- See NYSDOH AI guidelines Treatment of Alcohol Use Disorder and Treatment of Opioid Use Disorder, NYSDOH AI Clinical Guidance: Stimulant Use, and U.S. Public Health Service: A Clinical Practice Guideline for Treating Tobacco Use and Dependence.
Alcohol
In primary care settings, clinicians should screen all adult patients ≥18 years old for alcohol use. A large body of evidence indicates that screening tools can accurately identify unhealthy alcohol use (see Table 1: Recommended Validated Tools for Use in Medical Settings to Screen for Alcohol and Drug Use in Adults) and that brief counseling interventions can reduce alcohol use, improve health, and be cost-effective Patnode, et al. 2020; Kaner, et al. 2018; O'Connor, et al. 2018; O'Donnell, et al. 2014; McNeely, et al. 2008; Solberg, et al. 2008; Maciosek, et al. 2006. The National Committee on Quality Assurance adopted alcohol screening and brief intervention as a quality indicator in 2018 and incorporated it into the widely used Healthcare Effectiveness Data and Information Set performance measures.
In the absence of systematic screening, unhealthy alcohol use typically goes unidentified Hallgren, et al. 2022; McKnight-Eily, et al. 2020 or is identified by clinicians only when an individual has developed a severe alcohol use disorder or alcohol-related health problems, such as alcohol-related cirrhosis or pancreatitis.
| KEY POINTS |
|
Tobacco
Clinicians should screen all patients for all types of tobacco use, and when use is identified, provide counseling, assessment, and treatment Patnode, et al. 2021; USPSTF 2021. Every visit with a care provider allows for identifying a patient’s tobacco use and offering effective cessation interventions. Screening for tobacco use is often accomplished with 1 question: “Have you ever smoked cigarettes or used any other kind of tobacco?” Patients who answer “yes” should be asked about frequency and level of use in the past 30 days (e.g., number of cigarettes smoked per day) DHHS 2008. Despite concern about increasing rates of e-cigarette use, screening for electronic nicotine delivery systems is not currently a recommended practice Krist, et al. 2021; USPSTF 2021.
Other Drugs
Based on clinical experience and expertise and federal recommendations USPSTF(b) 2020, this committee recommends that clinicians screen for drug use other than alcohol and tobacco in adult patients ≥18 years old who present for primary care. Screening should be performed in settings where treatment or counseling resources are available on-site or by referral and should identify a patient’s use of illicitly manufactured drugs and nonmedical use of prescription drugs that can be misused (e.g., opioids, benzodiazepines, and stimulants).
Evidence supports the accuracy of validated screening questionnaires in adults Patnode, et al. 2020 and the benefits of pharmacologic treatment for opioid use disorder (OUD), which can be delivered effectively in primary care settings Wartko, et al. 2023 and no longer requires a waiver for prescribing buprenorphine Stringfellow, et al. 2021. However, data on the effectiveness of drug screening plus brief intervention to reduce drug use and associated health consequences are currently limited, and this is an area of ongoing research. Randomized controlled clinical trials have generated mixed results regarding the efficacy of brief interventions in reducing drug use Sahker, et al. 2022; Patnode, et al. 2020; Gelberg, et al. 2015; Roy-Byrne, et al. 2014; Saitz(a), et al. 2014; Humeniuk, et al. 2012. Evidence supporting drug interventions delivered in primary care has primarily come from treatment-seeking populations, rather than patients identified only through screening Saitz 2020; USPSTF(a) 2020.
No currently published studies demonstrate harms directly associated with screening adult primary care patients for drug use, although the potential for harm does exist Saitz 2020. For some patients, especially those who are pregnant or planning to conceive, positive results from a drug screening test could pose social or legal consequences, such as required reporting and the potential for involvement of child protective services (see discussion below). It is essential to respect the sensitivity of any substance use information documented in patients’ health records and ensure that patients understand privacy protections for their health information.
Rationale for drug use screening: This committee’s rationale for recommending drug use screening in adult patients, even with the potential for harm in some specific circumstances, is based on the following:
- Stigma is a significant barrier to identifying and treating unhealthy drug use or substance use disorders (SUDs). The exclusion of routine screening for drug use may perpetuate the perception that discussion of drug use with healthcare providers is taboo. This is especially the case if alcohol and tobacco use are discussed openly but drug use is not mentioned. Routine, matter-of-fact, nonjudgmental screening for drug use may help reduce stigma by normalizing this discussion.
- The social history that clinicians currently perform typically includes questions about alcohol, tobacco, and drug use but may not collect this information in a systematic and clinically useful manner. It is important that clinicians screen for drug use consistently, in a nonbiased manner, and use standardized, evidence-based screening tools.
- Fatal and non-fatal opioid overdose deaths can be reduced through increased identification of unhealthy opioid use and, when indicated, effective treatment with medications for OUD Watts, et al. 2022; Wakeman, et al. 2020; Sordo, et al. 2017; Cousins, et al. 2016.
- Identifying and addressing unhealthy drug use, including drug use disorders, may positively affect other patient outcomes. For instance, identification of benzodiazepine use in a patient receiving opioids for chronic pain could inform overdose prevention counseling, opioid prescribing, and provision of naloxone to reduce the patient’s overdose risk.
- Knowledge of a patient’s drug use is essential for accurate diagnosis and treatment. For example, in a patient who uses cocaine, chest pain could be the result of drug use rather than a blocked coronary artery, but without knowledge of the drug use, the clinician will not have the information necessary to perform the appropriate diagnostic workup. In addition, knowledge of drug use may be essential for an accurate diagnosis of psychiatric disorders, and knowledge of injection drug use can help guide screening for infections.
| KEY POINT |
|
Drug use screening in individuals who are pregnant or planning to conceive: Because there are potential legal and social consequences of a positive drug use screening result in individuals who are pregnant or planning to conceive, this committee urges caution when performing drug use screening. It is essential to engage patients in shared and informed decision-making before screening is performed. Fully informed consent includes clear discussion and confirmed patient understanding of the benefits, potential harms, and consequences of screening. For patients who are pregnant or planning to conceive, the informed consent discussion should include:
- Description of drug screening processes and procedures
- Potential benefits of drug screening for the patient
- Discussion of how results are interpreted and likely next steps if the screening result is positive
- Confirmation of confidentiality of the patient’s medical information
- Discussion of the risk of being reported to child protective services
- Discussion of the patient’s ability to refuse drug screening without repercussions, except in cases in which screening is mandated by an employer or by the court
- Psychosocial support and counseling about the potential harms of drugs and treatment options for SUD, if patients decline to be screened for other drugs
Screening to Inform Clinical Care
Screening is recommended for patients who use medications that have adverse interactions with alcohol or drugs. Iatrogenic harm is possible if a patient’s substance use is not identified, including adverse effects resulting from drug-medication interactions, overdose from combining prescribed medications with illicitly manufactured drugs, and withdrawal syndromes when a patient’s drug use is undisclosed and they are unable to use, such as during hospitalization Lindsey, et al. 2012; CDC 2007; Antoniou and Tseng 2002. Patients taking prescription opioids or benzodiazepines should be screened for use of alcohol and for illicitly manufactured or nonmedical use of other sedating drugs (including other opioids or benzodiazepines) that can increase the risk of overdose. Patients taking any controlled substances should be assessed for co-occurring substance use that may increase the probability of engaging in risky use of prescribed medications or of having or developing an SUD.
Clinicians should be aware of potential interactions between alcohol or drugs and medications, such as antiretroviral, pain management, or neurologic medications (e.g., gabapentin and pregabalin) Gomes, et al. 2017; Lyndon, et al. 2017; Lindsey, et al. 2012; Bruce, et al. 2008; Saitz 2005; Antoniou and Tseng 2002.
When counseling patients who use substances about drug-medication interactions, clinicians should be clear about the safety of their prescribed medications and be certain to encourage adherence to all critical medications, such as antiretroviral treatment Kalichman, et al. 2015.
See the following resources for checking drug-drug interactions:
- Drugs.com > Drug Interactions Checker
- University of Liverpool HEP Drug Interactions
- University of Liverpool HIV Drug Interactions
Clinicians should also perform substance use screening in patients who have symptoms or other medical conditions that could be caused or exacerbated by substance use, such as chest pain, liver disease, or mood disorders NIAAA 2024; Ries, et al. 2018; Kim, et al. 2017; Edelman and Fiellin 2016; Mertens, et al. 2005; Lock and Kaner 2004.
| Box 2: Implementing Substance Use Screening in Primary Care Settings |
|
Screening Tools
| RECOMMENDATION |
Screening Tools
|
Successful substance use screening relies on accurate patient self-report. Although urine toxicology, measures of blood alcohol level, or other laboratory testing may detect the presence of substances used very recently (typically hours or ≤4 days after the last use), these tests are not appropriate for identifying unhealthy use, which may be intermittent and occur over time Bosker and Huestis 2009; Cone and Huestis 2007; Verstraete 2004. Laboratory screening tests for alcohol and drugs do not provide information about the severity or consequences of use and thus provide less information than questionnaires.
No reliable biomarker with sufficient sensitivity and specificity identifies the range of drinking behaviors that constitute unhealthy alcohol use Afshar, et al. 2017; Jarvis, et al. 2017; Jatlow, et al. 2014; Stewart, et al. 2014; Verstraete 2004; Neumann and Spies 2003. For drug use, urine, saliva, and blood testing are not recommended as replacements for questionnaire-based screening because laboratory tests have a brief window of detection (typically 1 to 4 days) Bosker and Huestis 2009; Cone and Huestis 2007; Verstraete 2004. Although hair testing has a more extended detection period, the cost and lack of reliability for detecting occasional drug use decrease its utility in primary care Verstraete 2004.
Note:
|
||
| Table 1: Recommended Validated Tools for Use in Medical Settings to Screen for Alcohol and Drug Use in Adults [a] | ||
| Tool | Substance(s) Included | No. of Items, Approximate Time Required to Complete, and Format |
| AUDIT-C (Alcohol Use Disorders Identification Test-Concise) Bradley, et al. 2007; Bush, et al. 1998
|
Alcohol |
|
| SISQ-Alc (Single-Item Screening Questions for Alcohol) McNeely(c), et al. 2015; Smith, et al. 2009 |
Alcohol |
|
| SIS-C (Single-Item Screen-Cannabis) Matson, et al. 2022 |
Cannabis |
|
| SISQ-Drug (Single-Item Screening Questions for Drug Use) McNeely(c), et al. 2015; Smith, et al. 2010 |
Prescription drugs, other drugs |
|
| TAPS-1 (Tobacco, Alcohol, Prescription Medication, and Other Substance Use) Gryczynski, et al. 2017 |
Tobacco, alcohol, prescription drugs, other drugs |
|
| SUBS (Substance Use Brief Screen) McNeely(b) and Saitz 2015 |
Tobacco, alcohol, prescription drugs, other drugs |
|
| KEY POINT |
|
An optimal screening instrument will quickly and accurately identify individuals with the full spectrum of unhealthy use, fit into the existing clinical workflow, and have flexible administration options (i.e., self- or interviewer-administered). To facilitate patient reports of substance use, the language used in any screening tool should be clear and nonjudgmental. Drug screening should capture nonmedical prescription drug use and illicitly manufactured drug use. Table 1, above, lists recommended substance use screening tools.
The briefest approach to screening may be to use the Single-Item Screening Questions (SISQ) for alcohol or drug use (SISQ-Alc and SISQ-Drug). SISQ tools are validated for interviewer administration or patient administration and have good sensitivity and specificity. A positive response on SISQ tools identifies unhealthy use in the past year but does not indicate the level of risk. Both the Substance Use Brief Screen (SUBS) tool and the first section of the Tobacco, Alcohol, Prescription Medication, and Other Substance Use (TAPS-1) tool elicit information about use of tobacco, alcohol, illicitly manufactured drugs, and nonmedical prescription drugs through a single 4-item instrument. Like the SISQ-Alc and SISQ-Drug, the SUBS and TAPS-1 tools screen for any use in the past year, and a positive response indicates unhealthy use but does not identify level of risk. In states such as New York where cannabis is legal, asking about its use separately from that of illicitly manufactured drugs or nonmedical use of prescribed drugs may be preferable, and the Single-Item Screen-Cannabis, a validated single-item screening tool, is now available for this purpose Matson, et al. 2022; Sayre, et al. 2020.
Risk Assessment
| RECOMMENDATIONS |
Risk Assessment
|
Who to Assess
Clinicians should use validated tools to perform substance use assessments in individual patients who have any of the characteristics discussed below. The purpose of assessment is to identify the level of risk (low, moderate, or high) posed by a patient’s substance use to guide clinical decisions about intervention, treatment, and follow-up (see Figure 1: Substance Use Screening, Risk Assessment, Diagnosis, and Interventions). Clinicians experienced in assessing and treating SUD may elect to use the Diagnostic and Statistical Manual of Mental Disorders-5-TR criteria as the initial assessment tool.
Positive substance use screening test: Given current levels of substance use in the general population and the negative effects of unhealthy substance use, any positive screening test result should prompt an efficient and accurate risk assessment McNeely(a), et al. 2015; McNeely(c), et al. 2015.
Known history of SUD or overdose: Polysubstance use is common in people with SUD Ellis, et al. 2023; Karamouzian, et al. 2022; Lin, et al. 2021; John, et al. 2018; Falk, et al. 2006. For patients with a history of SUD, identification of all substances used, including tobacco, and assessment of the associated levels of risk are indicated for early intervention and clinical decision-making. SUDs are chronic conditions, and even patients with long periods of abstinence remain vulnerable to resuming previous patterns of use McLellan, et al. 2000. Patients with a history of SUD may reduce or stop use of one substance but develop unhealthy use of a different substance (e.g., alcohol) Lin, et al. 2021; Callaghan, et al. 2018; Wang, et al. 2017; Falk, et al. 2006; Earleywine and Newcomb 1997. Overdose is frequently the result of polysubstance use, and use of fentanyl and stimulants (methamphetamine, cocaine) is driving unprecedented rates of overdose death Ciccarone 2021; Cicero, et al. 2020. The use of opioids in combination with alcohol or benzodiazepines also puts individuals at high risk of overdose Tori, et al. 2020. In patients with a history of nonfatal overdose, it is critically important to conduct an assessment and identify all of the substances being used; the results will guide education and treatment to reduce the risk of another overdose.
The level of risk of associated with substance use in individuals who are planning to become pregnant should guide clinician counseling, particularly in light of the risk of fetal alcohol spectrum disorder that occurs early in pregnancy May, et al. 2018; Moyer 2013; Stade, et al. 2009; Floyd, et al. 2008; Floyd, et al. 2006; DHHS 2005; CDC 2003. In addition, it is reasonable to perform a substance use assessment in patients with chronic diseases who have difficulty following through with treatment recommendations or are not responding as expected to treatment of their medical condition Garin, et al. 2017; Daskalopoulou, et al. 2014.
Risk Assessment Tools
Substance use assessment tools are designed to collect information on the quantity, frequency, and duration of substance use and to indicate a risk level (see Table 2, below).
Notes:
|
||
| Table 2: Brief, Validated Risk Assessment Tools for Use in Medical Settings With Adults ≥18 Years Old [a] | ||
| Tool | Substance(s) Included | No. of Items, Approximate Time Required to Complete, and Format |
| ASSIST (Alcohol, Smoking, and Substance Involvement Screening Test) Humeniuk, et al. 2008
|
Tobacco, alcohol, prescription drugs, and other drugs; identifies specific drug classes |
|
| TAPS-2 (Tobacco, Alcohol, Prescription Medication, and Other Substance Use) [b] Adam, et al. 2019; McNeely(a), et al. 2016 |
Tobacco, alcohol, prescription drugs, other drugs; identifies specific drug classes |
|
| ACASI-ASSIST (Audio Computer-Assisted Self-Interview-ASSIST) Kumar, et al. 2016; McNeely(b), et al. 2016 |
Tobacco, alcohol, prescription drugs, and other drugs; identifies specific drug classes |
|
| Alcohol Symptom Checklist Hallgren, et al. 2022 |
Alcohol |
|
| AUDIT (Alcohol Use Disorders Identification Test) [c] Reinert and Allen 2007
|
Alcohol |
|
| DUDIT (Drug Use Disorders Identification Test) Hildebrand 2015; Berman, et al. 2005
|
All drugs; does not identify drug classes |
|
| DAST-10 (Drug Abuse Screening Test) Yudko, et al. 2007; Skinner 1982
|
All drugs; does not identify drug classes |
|
Patient Engagement and Interventions
| RECOMMENDATIONS |
Patient Engagement
Interventions
|
Abbreviations: DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; SUD, substance use disorder. |
Many individuals with unhealthy alcohol use or other substance use regularly interact with the healthcare system, and primary care providers are optimally positioned to offer prevention, risk reduction, and treatment interventions. Routine screening and annual rescreening provide structure and opportunity to identify at-risk individuals, monitor for significant changes, and revisit identified concerns.
The Screening, Brief Intervention, and Referral to Treatment (SBIRT) framework provides a comprehensive approach to the delivery of early intervention and treatment services for patients with unhealthy substance use of various degrees of severity. The key elements include:
- Screening/risk assessment to quickly identify at-risk individuals
- Brief intervention focused on increasing awareness and motivation toward behavioral change
- Referral to treatment to facilitate access to care
For additional guidance on implementation and reimbursement based on this framework, see Substance Abuse and Mental Health Services Administration (SAMHSA): Screening, Brief Intervention, and Referral to Treatment (SBIRT) and Box 2: Implementing Substance Use Screening in Primary Care Settings.
Patient Engagement
A positive substance use screening result should trigger further risk assessment, including a detailed history and understanding of individual risk factors; see guideline section Risk Assessment. Assessment tools determine the level of risk (low-, moderate-, and high-risk use) and thus the potential for negative consequences and appropriate interventions. Figure 1: Substance Use Screening, Risk Assessment, Diagnosis, and Interventions outlines the sequence of steps for the clinician.
When administering a risk assessment tool or during patient evaluation after a self-administered risk assessment, clinicians should remain alert to the patient’s perception of their substance use and readiness to change behaviors. Based on clinical experience, this interaction is an important opportunity to build rapport, dispel misconceptions, and engage patients in a therapeutic relationship. Understanding a patient’s readiness to change and identifying internal motivators for change provide important building blocks to shape the intervention strategy.
Motivational interviewing: Interventions tailored to match a patient’s level of risk, perception of their substance use, and readiness to change can promote engagement and increase the probability of progress toward goals VA/DoD 2015; SAMHSA 1997. The principals of motivational interviewing (MI) provide a framework for this approach, and all clinicians can develop the skills to educate, advise, offer treatment, or refer patients for appropriate interventions McLellan 2017; Edelman and Fiellin 2016. The core skills of MI, as defined by Miller and Rollnick, can be remembered with the acronym OARS, which stands for: open-ended questioning, affirming, reflective listening, and summarizing Miller and Rollnick 2013. For more information, see Resources box, below.
Trauma-informed care: Individuals with SUD have a high prevalence of childhood trauma Bartholow and Huffman 2023; Karsberg, et al. 2021; Zarse, et al. 2019, and substance use is a risk factor for repeated exposure to traumatic events Aronowitz and Meisel 2022; Simon, et al. 2020. Knowing that trauma contributes to challenges connecting to the healthcare system, clinicians and organizations with a trauma-informed approach can better overcome these barriers and improve outcomes. For more information on trauma-informed care, see the Resources box, below.
| RESOURCES |
|
Interventions
Positive reinforcement (for patients with low-risk substance use): For alcohol use, reinforce the benefits of staying below the U.S. Department of Health and Human Services and Department of Agriculture 2015-2020 Dietary Guidelines (1 drink or fewer per day for women and 2 drinks or fewer per day for men). Statements such as “The amount that you are drinking falls within a level that is considered safe for most healthy adults and is unlikely to have a negative impact on your health” and “In general, the less you drink, the better it is for your health” reinforce low-risk alcohol use. Be alert to pregnancy, older age (>65 years), and other health conditions that may warrant advice to drink less or not at all.
Brief advice (for patients with moderate- or high-risk substance use): Statements such as “As your healthcare provider, I am concerned about your alcohol (or substance) use and the potential impact on your health” and discussion of any related health effects (current or potential) should be integrated into the visit. This discussion can be supplemented by additional interventions as time and resources allow.
For individuals who use alcohol, clinicians can provide information on the recommended safe limits of use. Safe limits have not been established for older individuals or those with medical or psychiatric comorbidities. If a patient is hesitant, negotiate an individualized goal. Little information is available about the dose limits and associated health risks of cannabis and illicitly manufactured drugs.
Harm reduction strategies (for patients with moderate- or high-risk substance use): See the NYSDOH AI guideline Substance Use Harm Reduction in Medical Care for more information, including resources in New York State.
Overdose prevention strategies: Counsel patients to:
- Assume all illicitly manufactured opioids will contain fentanyl or other high-potency synthetic opioids and that stimulants and counterfeit pills may contain these agents.
- When possible, test drugs with fentanyl test strips or other drug-checking systems. Online sources include MATTERS (for New York State residents and programs, no charge), DanceSafe, and BTNX. Some NYS Authorized Syringe Exchange Sites may provide fentanyl test strips and other drug-checking systems.
- Try to avoid using drugs alone, and if they have to use alone, arrange for someone to check in or use phone- and web-based apps (e.g., Never Use Alone Inc. at 800-484-3731).
- When using any drug, start with a small amount.
- Carry naloxone (NLX), learn how to use it to reverse an opioid overdose, and encourage friends and contacts to do the same. The 4 mg NLX nasal spray formulation is available at pharmacies, at NYSDOH-Registered Opioid Overdose Prevention Programs (no charge), and through online resources such as NEXT Distro. NLX is covered by NYS Medicaid and most private insurers.
Brief interventions (for patients with moderate-risk substance use or high-risk substance use not diagnosed as a use disorder): A brief intervention is a time-limited, patient-centered strategy that focuses on increasing insight and awareness about substance use and motivation toward behavioral change. Brief interventions can range from 5 to 20 minutes in duration, vary in frequency, and include a variety of components. Common elements of a brief intervention include discussion of the risks and rewards of substance use as perceived by the patient and individualized feedback about the level of risk.
Using these techniques, clinicians can encourage “change talk” by amplifying statements about a patient’s desire, ability, and reasons for change Rollnick, et al. 2022. The amount of time spent in change talk is correlated with improved outcomes; the more a patient verbalizes their desire and reasons for change, the more likely it is to happen.
Robust evidence supports the efficacy of brief advice and other brief interventions in the primary care setting for reducing alcohol use among individuals with unhealthy use who do not meet the criteria for alcohol use disorder Curry, et al. 2018; Kaner, et al. 2018; O'Connor, et al. 2018. However, the optimal timing, dose, and order of interventions is unknown. A systematic review of the literature on brief alcohol intervention implementation in medical settings was unable to identify specific interventions that were clearly associated with improved outcomes Curry, et al. 2018. The most common component was the use of personalized feedback in which participants were shown how their alcohol use compared with that of others. Personalized feedback was often combined with MI or other strategies, such as drinking diaries, action plans, or alcohol use “prescriptions.”
Randomized controlled clinical trials have generated mixed results regarding the efficacy of brief interventions in reducing drug use Sahker, et al. 2022; Patnode, et al. 2020; Gelberg, et al. 2015; Roy-Byrne, et al. 2014; Saitz(a), et al. 2014; Humeniuk, et al. 2012. Evidence supporting drug use interventions delivered in primary care has primarily come from treatment-seeking populations rather than patients identified only through screening Saitz 2020; USPSTF(a) 2020. However, brief interventions are recommended by SAMHSA and have been implemented in many healthcare settings with no evidence of harm SAMHSA 2018.
In the absence of evidence to guide the choice of specific interventions, clinicians should engage in any strategies that are available and feasible. Clinician factors, including training and time restrictions, will guide strategy. Practice factors, including standard workflows, electronic health record decision support, and availability of integrated behavioral health specialists, can enhance the uptake and implementation of best practices Loughran, et al. 2021.
Individualized Follow-Up
Because substance use behaviors can change over time, annual rescreening is recommended for individuals with low-risk substance use. For individuals with moderate- or high-risk substance use and those meeting criteria for an SUD, the frequency and type of follow-up will be individualized. As with other chronic diseases, the plan will vary based on the severity of the problem, presence of significant medical or psychiatric comorbidities, and the patient’s perception and goals. When indicated, the plan should include referral for specialty services.
Diagnosis of Substance Use Disorder
| RECOMMENDATIONS |
Diagnosis of SUD
Treatment
|
Abbreviations: DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; SUD, substance use disorder. Note:
|
The diagnosis of an SUD and its severity is made by a clinical interview and based on DSM-5-TR diagnostic criteria (see Table 3, below) APA 2022. Diagnostic checklists incorporated into the health record can be helpful tools. Studies have confirmed that symptom checklists can reliably assess for alcohol use disorder criteria in patients who screen positive for high-risk drinking Hallgren, et al. 2022; a similar strategy may be useful for the diagnosis of other SUDs Matson, et al. 2023.
Individuals with a diagnosis of SUD should be offered pharmacologic and behavioral treatment as indicated and available (see Note [a], above). Conversations about treatment options should be guided by precepts outlined in the guideline section Patient Engagement. When referral to specialty addiction treatment is necessary, primary care providers can support patients in selecting treatment resources, navigating potential barriers, and checking in about progress while continuing to address medical needs.
Patients often present with concurrent SUDs and mental health disorders NIDA 2020. Symptoms of one can mimic the other, making it challenging to arrive at a definitive diagnosis SAMHSA 2019. Clinicians should consider a diagnosis of SUD before establishing a primary psychiatric diagnosis (e.g., alcohol-induced depressive disorder vs. major depressive disorder). Symptoms of intoxication, such as mood changes or perceptual disturbances, and symptoms of withdrawal, such as depression, anxiety, irritability, and insomnia, can also mimic psychiatric disorders and should be carefully assessed. Care providers should consult with a mental health specialist when symptoms are severe and/or when a clear diagnosis is difficult to establish.
| Abbreviations: DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; SUD, substance use disorder.
Notes: |
|
| Table 3: DSM-5-TR Criteria for Diagnosing and Classifying Substance Use Disorders [a,b] | |
| Criteria Type | Description |
| Impaired control over substance use (DSM-5-TR criteria 1 to 4) |
|
| Social impairment (DSM-5-TR criteria 5 to 7) |
|
| Risky use (DSM-5-TR criteria 8 and 9) |
|
| Pharmacologic (DSM-5-TR criteria 10 and 11) |
|
All Recommendations
| ALL RECOMMENDATIONS: SUBSTANCE USE SCREENING, RISK ASSESSMENT, AND USE DISORDER DIAGNOSIS IN ADULTS |
Screening
Screening Tools
Risk Assessment
Patient Engagement
Interventions
Diagnosis of SUD
Treatment
|
Abbreviations: DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision; SUD, substance use disorder. Note:
|
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
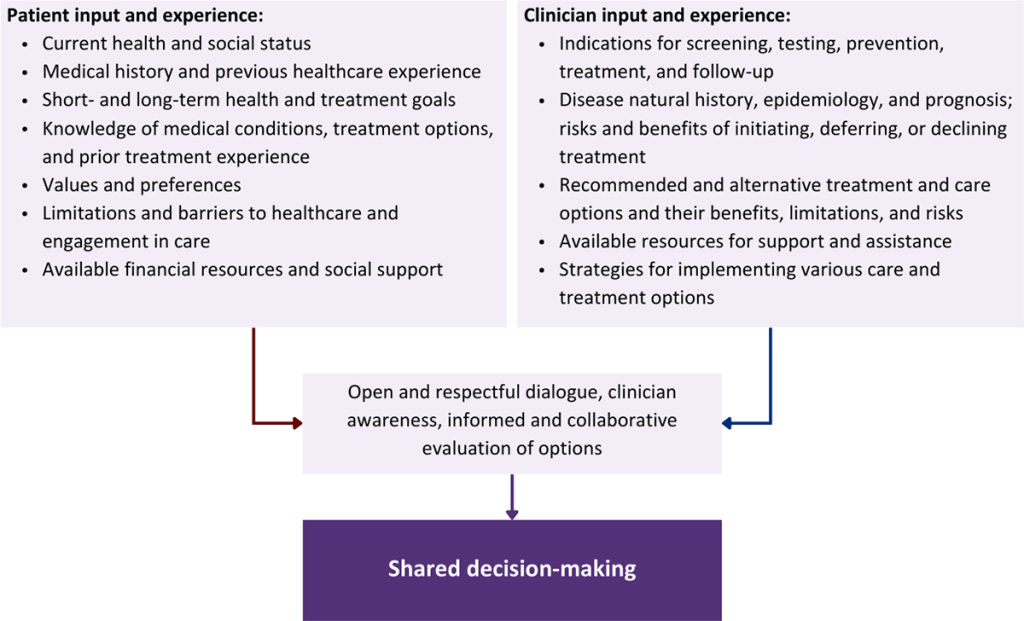
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Adam A., Schwartz R. P., Wu L. T., et al. Electronic self-administered screening for substance use in adult primary care patients: feasibility and acceptability of the tobacco, alcohol, prescription medication, and other substance use (myTAPS) screening tool. Addict Sci Clin Pract 2019;14(1):39. [PMID: 31615549]
Afshar M., Burnham E. L., Joyce C., et al. Cut-point levels of phosphatidylethanol to identify alcohol misuse in a mixed cohort including critically ill patients. Alcohol Clin Exp Res 2017;41(10):1745-53. [PMID: 28792620]
Antoniou T., Tseng A. L. Interactions between recreational drugs and antiretroviral agents. Ann Pharmacother 2002;36(10):1598-1613. [PMID: 12243611]
APA. Diagnostic and statistical manual of mental disorders, fifth edition, text revision; 2022; Washington, DC. https://dsm.psychiatryonline.org/doi/book/10.1176/appi.books.9780890425787
Aronowitz S., Meisel Z. F. Addressing stigma to provide quality care to people who use drugs. JAMA Netw Open 2022;5(2):e2146980. [PMID: 35119465]
Bartholow L. A., Huffman R. T. The necessity of a trauma-informed paradigm in substance use disorder services. J Am Psychiatr Nurses Assoc 2023;29(6):470-76. [PMID: 34334012]
Berman, A. H.. Drug Use Disorders Identification Test (DUDIT). 2005 Mar 1. https://www.emcdda.europa.eu/drugs-library/drug-use-disorders-identification-test-dudit_en [accessed 2024 Mar 20]
Bosker W. M., Huestis M. A. Oral fluid testing for drugs of abuse. Clin Chem 2009;55(11):1910-31. [PMID: 19745062]
Bradley K. A., DeBenedetti A. F., Volk R. J., et al. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res 2007;31(7):1208-17. [PMID: 17451397]
Bradley K. A., Lapham G. T., Hawkins E. J., et al. Quality concerns with routine alcohol screening in VA clinical settings. J Gen Intern Med 2011;26(3):299-306. [PMID: 20859699]
Bradley K. A., Lapham G. T., Lee A. K. Screening for drug use in primary care: practical implications of the new USPSTF recommendation. JAMA Intern Med 2020;180(8):1050-51. [PMID: 32515790]
Bruce R. D., Altice F. L., Friedland G. H. Pharmacokinetic drug interactions between drugs of abuse and antiretroviral medications: implications and management for clinical practice. Expert Rev Clin Pharmacol 2008;1(1):115-27. [PMID: 24410515]
Bush K., Kivlahan D. R., McDonell M. B., et al. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med 1998;158(16):1789-95. [PMID: 9738608]
Callaghan R. C., Gatley J. M., Sykes J., et al. The prominence of smoking-related mortality among individuals with alcohol- or drug-use disorders. Drug Alcohol Rev 2018;37(1):97-105. [PMID: 28009934]
CDC. Motivational intervention to reduce alcohol-exposed pregnancies--Florida, Texas, and Virginia, 1997-2001. MMWR Morb Mortal Wkly Rep 2003;52(19):441-44. [PMID: 12807086]
CDC. Unintentional poisoning deaths--United States, 1999-2004. MMWR Morb Mortal Wkly Rep 2007;56(5):93-96. [PMID: 17287712]
CDC. Alcohol-Related Disease Impact (ARDI) application. 2022. https://nccd.cdc.gov/DPH_ARDI/default/default.aspx [accessed 2024 Jan 16]
CDC. National Vital Statistics System: provisional drug overdose death counts. 2024 May 15. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm [accessed 2024 Jan 16]
Ciccarone D. The rise of illicit fentanyls, stimulants and the fourth wave of the opioid overdose crisis. Curr Opin Psychiatry 2021;34(4):344-50. [PMID: 33965972]
Cicero T. J., Ellis M. S., Kasper Z. A. Polysubstance use: a broader understanding of substance use during the opioid crisis. Am J Public Health 2020;110(2):244-50. [PMID: 31855487]
CMS. 2014 Clinical Quality Measures (CQMs): adult recommended core measures. 2013 Jan. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_CQM_AdultRecommend_CoreSetTable.pdf [accessed 2020 Mar 31]
Cone E. J., Huestis M. A. Interpretation of oral fluid tests for drugs of abuse. Ann N Y Acad Sci 2007;1098:51-103. [PMID: 17332074]
Cousins G., Boland F., Courtney B., et al. Risk of mortality on and off methadone substitution treatment in primary care: a national cohort study. Addiction 2016;111(1):73-82. [PMID: 26234389]
Curry S. J., Krist A. H., Owens D. K., et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: US Preventive Services Task Force recommendation statement. JAMA 2018;320(18):1899-1909. [PMID: 30422199]
Daskalopoulou M., Rodger A., Phillips A. N., et al. Recreational drug use, polydrug use, and sexual behaviour in HIV-diagnosed men who have sex with men in the UK: results from the cross-sectional ASTRA study. Lancet HIV 2014;1(1):e22-31. [PMID: 26423813]
DHHS. U.S. Surgeon General releases advisory on alcohol use in pregnancy. 2005 Feb 21. http://come-over.to/FAS/SurGenAdvisory.htm [accessed 2020 Mar 31]
DHHS. Helping smokers quit: a guide for clinicians. 2008 May. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/clinicians-providers/guidelines-recommendations/tobacco/clinicians/references/clinhlpsmkqt/clinhlpsmksqt.pdf [accessed 2020 Mar 31]
Earleywine M., Newcomb M. D. Concurrent versus simultaneous polydrug use: prevalence, correlates, discriminant validity, and prospective effects on health outcomes. Exp Clin Psychopharmacol 1997;5(4):353-64. [PMID: 9386962]
Edelman E. J., Fiellin D. A. In the clinic. Alcohol use. Ann Intern Med 2016;164(1):ITC1-16. [PMID: 26747315]
Ellis J. D., Rabinowitz J. A., Ware O. D., et al. Patterns of polysubstance use and clinical comorbidity among persons seeking substance use treatment: An observational study. J Subst Use Addict Treat 2023;146:208932. [PMID: 36880895]
Falk D. E., Yi H. Y., Hiller-Sturmhöfel S. An epidemiologic analysis of co-occurring alcohol and tobacco use and disorders: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Alcohol Res Health 2006;29(3):162-71. [PMID: 17373404]
Floyd R. L., Jack B. W., Cefalo R., et al. The clinical content of preconception care: alcohol, tobacco, and illicit drug exposures. Am J Obstet Gynecol 2008;199(6 Suppl 2):s333-39. [PMID: 19081427]
Floyd R. L., O'Connor M. J., Bertrand J., et al. Reducing adverse outcomes from prenatal alcohol exposure: a clinical plan of action. Alcohol Clin Exp Res 2006;30(8):1271-75. [PMID: 16899029]
Garin N., Zurita B., Velasco C., et al. Prevalence and clinical impact of recreational drug consumption in people living with HIV on treatment: a cross-sectional study. BMJ Open 2017;7(1):e014105. [PMID: 28100565]
GBD. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018;5(12):987-1012. [PMID: 30392731]
Gelberg L., Andersen R. M., Afifi A. A., et al. Project QUIT (Quit Using Drugs Intervention Trial): a randomized controlled trial of a primary care-based multi-component brief intervention to reduce risky drug use. Addiction 2015;110(11):1777-90. [PMID: 26471159]
Gomes T., Juurlink D. N., Antoniou T., et al. Gabapentin, opioids, and the risk of opioid-related death: a population-based nested case-control study. PLoS Med 2017;14(10):e1002396. [PMID: 28972983]
Gomes T., Ledlie S., Tadrous M., et al. Trends in opioid toxicity-related deaths in the US before and after the start of the COVID-19 pandemic, 2011-2021. JAMA Netw Open 2023;6(7):e2322303. [PMID: 37418260]
Gordon A. J., Bertholet N., McNeely J., et al. 2013 update in addiction medicine for the generalist. Addict Sci Clin Pract 2013;8(1):18. [PMID: 24499640]
Gryczynski J., McNeely J., Wu L. T., et al. Validation of the TAPS-1: a four-item screening tool to identify unhealthy substance use in primary care. J Gen Intern Med 2017;32(9):990-96. [PMID: 28550609]
Hallgren K. A., Matson T. E., Oliver M., et al. Practical assessment of DSM-5 alcohol use disorder criteria in routine care: high test-retest reliability of an alcohol symptom checklist. Alcohol Clin Exp Res 2022;46(3):458-67. [PMID: 35275415]
Hallgren K. A., Witwer E., West I., et al. Prevalence of documented alcohol and opioid use disorder diagnoses and treatments in a regional primary care practice-based research network. J Subst Abuse Treat 2020;110:18-27. [PMID: 31952624]
Hildebrand M. The psychometric properties of the Drug Use Disorders Identification Test (DUDIT): a review of recent research. J Subst Abuse Treat 2015;53:52-59. [PMID: 25682718]
Humeniuk R., Ali R., Babor T., et al. A randomized controlled trial of a brief intervention for illicit drugs linked to the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in clients recruited from primary health-care settings in four countries. Addiction 2012;107(5):957-66. [PMID: 22126102]
Humeniuk R., Ali R., Babor T. F., et al. Validation of the Alcohol, Smoking And Substance Involvement Screening Test (ASSIST). Addiction 2008;103(6):1039-47. [PMID: 18373724]
Jarvis M., Williams J., Hurford M., et al. Appropriate use of drug testing in clinical addiction medicine. J Addict Med 2017;11(3):163-73. [PMID: 28557958]
Jatlow P. I., Agro A., Wu R., et al. Ethyl glucuronide and ethyl sulfate assays in clinical trials, interpretation, and limitations: results of a dose ranging alcohol challenge study and 2 clinical trials. Alcohol Clin Exp Res 2014;38(7):2056-65. [PMID: 24773137]
John W. S., Zhu H., Mannelli P., et al. Prevalence, patterns, and correlates of multiple substance use disorders among adult primary care patients. Drug Alcohol Depend 2018;187:79-87. [PMID: 29635217]
Jonas D. E., Amick H. R., Feltner C., et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA 2014;311(18):1889-1900. [PMID: 24825644]
Kalichman S. C., Kalichman M. O., Cherry C., et al. Intentional medication nonadherence because of interactive toxicity beliefs among HIV-positive active drug users. J Acquir Immune Defic Syndr 2015;70(5):503-9. [PMID: 26226250]
Kaner E. F., Beyer F. R., Muirhead C., et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev 2018;2(2):CD004148. [PMID: 29476653]
Karamouzian M., Pilarinos A., Hayashi K., et al. Latent patterns of polysubstance use among people who use opioids: a systematic review. Int J Drug Policy 2022;102:103584. [PMID: 35074608]
Karsberg S., Hesse M., Pedersen M. M., et al. The impact of poly-traumatization on treatment outcomes in young people with substance use disorders. BMC Psychiatry 2021;21(1):140. [PMID: 33685430]
Kim T. W., Bernstein J., Cheng D. M., et al. Receipt of addiction treatment as a consequence of a brief intervention for drug use in primary care: a randomized trial. Addiction 2017;112(5):818-27. [PMID: 27886657]
Krist A. H., Davidson K. W., Mangione C. M., et al. Interventions for tobacco smoking cessation in adults, including pregnant persons: US Preventive Services Task Force recommendation statement. JAMA 2021;325(3):265-79. [PMID: 33464343]
Kumar P. C., Cleland C. M., Gourevitch M. N., et al. Accuracy of the Audio Computer Assisted Self Interview version of the Alcohol, Smoking and Substance Involvement Screening Test (ACASI ASSIST) for identifying unhealthy substance use and substance use disorders in primary care patients. Drug Alcohol Depend 2016;165:38-44. [PMID: 27344194]
Lin L. A., Bohnert A. S., Blow F. C., et al. Polysubstance use and association with opioid use disorder treatment in the US Veterans Health Administration. Addiction 2021;116(1):96-104. [PMID: 32428386]
Lindsey W. T., Stewart D., Childress D. Drug interactions between common illicit drugs and prescription therapies. Am J Drug Alcohol Abuse 2012;38(4):334-43. [PMID: 22221229]
Lock C. A., Kaner E. F. Implementation of brief alcohol interventions by nurses in primary care: do non-clinical factors influence practice?. Fam Pract 2004;21(3):270-75. [PMID: 15128688]
Loughran T. A., Scharer J. L., Rodriguez L., et al. Brief alcohol interventions in U.S. medical settings: a systematic review of the implementation literature. J Subst Abuse Treat 2021;131:108456. [PMID: 34098287]
Lyndon A., Audrey S., Wells C., et al. Risk to heroin users of polydrug use of pregabalin or gabapentin. Addiction 2017;112(9):1580-89. [PMID: 28493329]
Maciosek M. V., Coffield A. B., Edwards N. M., et al. Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med 2006;31(1):52-61. [PMID: 16777543]
Matson Theresa E., Hallgren Kevin A., Lapham Gwen T., et al. Psychometric performance of a substance use symptom checklist to help clinicians assess substance use disorder in primary pare. JAMA Network Open 2023;6(5):e2316283. https://doi.org/10.1001/jamanetworkopen.2023.16283
Matson T. E., Lapham G. T., Bobb J. F., et al. Validity of the Single-Item Screen-Cannabis (SIS-C) for cannabis use disorder screening in routine care. JAMA Netw Open 2022;5(11):e2239772. [PMID: 36318205]
Mattick R. P., Breen C., Kimber J., et al. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev 2014;2014(2):CD002207. [PMID: 24500948]
May P. A., Chambers C. D., Kalberg W. O., et al. Prevalence of fetal alcohol spectrum disorders in 4 US communities. JAMA 2018;319(5):474-82. [PMID: 29411031]
McKnight-Eily L. R., Okoro C. A., Turay K., et al. Screening for alcohol use and brief counseling of adults - 13 states and the District of Columbia, 2017. MMWR Morb Mortal Wkly Rep 2020;69(10):265-70. [PMID: 32163383]
McLellan A. T. Substance misuse and substance use disorders: why do they matter in healthcare?. Trans Am Clin Climatol Assoc 2017;128:112-30. [PMID: 28790493]
McLellan A. T., Lewis D. C., O'Brien C. P., et al. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA 2000;284(13):1689-95. [PMID: 11015800]
McNeely J., Adam A., Rotrosen J., et al. Comparison of methods for alcohol and drug screening in primary care clinics. JAMA Netw Open 2021;4(5):e2110721. [PMID: 34014326]
McNeely J., Kumar P. C., Rieckmann T., et al. Barriers and facilitators affecting the implementation of substance use screening in primary care clinics: a qualitative study of patients, providers, and staff. Addict Sci Clin Pract 2018;13(1):8. [PMID: 29628018]
McNeely J., Windham B. G., Anderson D. E. Dietary sodium effects on heart rate variability in salt sensitivity of blood pressure. Psychophysiology 2008;45(3):405-11. [PMID: 18047481]
McNeely(a) J., Strauss S. M., Saitz R., et al. A brief patient self-administered substance use screening tool for primary care: two-site validation study of the Substance Use Brief Screen (SUBS). Am J Med 2015;128(7):784.e9-19. [PMID: 25770031]
McNeely(a) J., Wu L. T., Subramaniam G., et al. Performance of the Tobacco, Alcohol, Prescription medication, and other Substance use (TAPS) tool for substance use screening in primary care patients. Ann Intern Med 2016;165(10):690-99. [PMID: 27595276]
McNeely(b) J., Saitz R. Appropriate screening for substance use vs disorder. JAMA Intern Med 2015;175(12):1997-98. [PMID: 26641355]
McNeely(b) J., Strauss S. M., Rotrosen J., et al. Validation of an Audio Computer-Assisted Self-Interview (ACASI) version of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in primary care patients. Addiction 2016;111(2):233-44. [PMID: 26360315]
McNeely(c) J., Cleland C. M., Strauss S. M., et al. Validation of Self-Administered Single-Item Screening Questions (SISQs) for unhealthy alcohol and drug use in primary care patients. J Gen Intern Med 2015;30(12):1757-64. [PMID: 25986138]
Mertens J. R., Weisner C., Ray G. T., et al. Hazardous drinkers and drug users in HMO primary care: prevalence, medical conditions, and costs. Alcohol Clin Exp Res 2005;29(6):989-98. [PMID: 15976525]
Miller P. M., Thomas S. E., Mallin R. Patient attitudes towards self-report and biomarker alcohol screening by primary care physicians. Alcohol Alcohol 2006;41(3):306-10. [PMID: 16574672]
Miller W. R., Rollnick S. Motivational interviewing: helping people change. Guilford Press; 2013; New York (NY).
Moyer V. A. Screening and behavioral counseling interventions in primary care to reduce alcohol misuse: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2013;159(3):210-18. [PMID: 23698791]
Neumann T., Spies C. Use of biomarkers for alcohol use disorders in clinical practice. Addiction 2003;98 Suppl 2:81-91. [PMID: 14984245]
NIAAA. The healthcare professional's core resource on alcohol. 2024 Mar 13. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol [accessed 2024 Jan 16]
NIDA. Screening for drug use in general medical settings: quick reference guide. 2011 Dec. https://nida.nih.gov/sites/default/files/pdf/screening_qr.pdf [accessed 2020 Mar 31]
NIDA. Common comorbidities with substance use disorders research report. 2020 Apr. https://www.ncbi.nlm.nih.gov/books/NBK571451/ [accessed 2024 Feb 8]
O'Connor E. A., Perdue L. A., Senger C. A., et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2018;320(18):1910-28. [PMID: 30422198]
O'Donnell A., Anderson P., Newbury-Birch D., et al. The impact of brief alcohol interventions in primary healthcare: a systematic review of reviews. Alcohol Alcohol 2014;49(1):66-78. [PMID: 24232177]
Patnode C. D., Henderson J. T., Coppola E. L., et al. Interventions for tobacco cessation in adults, including pregnant persons: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2021;325(3):280-98. [PMID: 33464342]
Patnode C. D., Perdue L. A., Rushkin M., et al. Screening for unhealthy drug use: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2020;323(22):2310-28. [PMID: 32515820]
Reinert D. F., Allen J. P. The Alcohol Use Disorders Identification Test: an update of research findings. Alcohol Clin Exp Res 2007;31(2):185-99. [PMID: 17250609]
Ries R. K., Fiellin D. A., Miller S. C., et al. The ASAM principles of addiction medicine. Wolters Kluwer; 2018. https://shop.lww.com/The-ASAM-Principles-of-Addiction-Medicine/p/9781496371010
Rollnick S., Miller W. R., Butler C. C. Motivational interviewing in health care: helping patients change behavior. Guilford Press; 2022; New York (NY).
Roy-Byrne P., Bumgardner K., Krupski A., et al. Brief intervention for problem drug use in safety-net primary care settings: a randomized clinical trial. JAMA 2014;312(5):492-501. [PMID: 25096689]
Sahker E., Luo Y., Sakata M., et al. Efficacy of brief intervention for unhealthy drug use in outpatient medical care: a systematic review and meta-analysis. J Gen Intern Med 2022;37(8):2041-49. [PMID: 35419744]
Saitz R. Clinical practice. Unhealthy alcohol use. N Engl J Med 2005;352(6):596-607. [PMID: 15703424]
Saitz R. Screening for unhealthy drug use: neither an unreasonable idea nor an evidence-based practice. JAMA 2020;323(22):2263-65. [PMID: 32515804]
Saitz(a) R., Palfai T. P., Cheng D. M., et al. Screening and brief intervention for drug use in primary care: the ASPIRE randomized clinical trial. JAMA 2014;312(5):502-13. [PMID: 25096690]
Saitz(b) R., Cheng D. M., Allensworth-Davies D., et al. The ability of single screening questions for unhealthy alcohol and other drug use to identify substance dependence in primary care. J Stud Alcohol Drugs 2014;75(1):153-57. [PMID: 24411807]
SAMHSA. A guide to substance abuse services for primary care clinicians. 1997. https://www.ncbi.nlm.nih.gov/books/NBK64827/ [accessed 2020 Mar 31]
SAMHSA. Implementing care for alcohol & other drug use in medical settings: an extension of SBIRT. SBIRT change guide 1.0. 2018 Feb. https://www.thenationalcouncil.org/wp-content/uploads/2021/04/Implementing_Care_for_Alcohol_and_Other_Drug_Use_In_Medical_Settings_-_An_Extension_of_SBIRT.pdf [accessed 2020 Mar 31]
SAMHSA. Key substance use and mental health indicators in the United States: results from the 2018 National Survey on Drug Use and Health. 2019 Aug. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHNationalFindingsReport2018/NSDUHNationalFindingsReport2018.pdf [accessed 2020 Jan 6]
Sayre M., Lapham G. T., Lee A. K., et al. Routine assessment of symptoms of substance use disorders in primary care: prevalence and severity of reported symptoms. J Gen Intern Med 2020;35(4):1111-19. [PMID: 31974903]
Schulden J. D., Thomas Y. F., Compton W. M. Substance abuse in the United States: findings from recent epidemiologic studies. Curr Psychiatry Rep 2009;11(5):353-59. [PMID: 19785975]
Simon R., Snow R., Wakeman S. Understanding why patients with substance use disorders leave the hospital against medical advice: a qualitative study. Subst Abus 2020;41(4):519-25. [PMID: 31638862]
Simonetti J. A., Lapham G. T., Williams E. C. Association between receipt of brief alcohol intervention and quality of care among veteran outpatients with unhealthy alcohol use. J Gen Intern Med 2015;30(8):1097-1104. [PMID: 25691238]
Skinner H. A. The drug abuse screening test. Addict Behav 1982;7(4):363-71. [PMID: 7183189]
Smith P. C., Schmidt S. M., Allensworth-Davies D., et al. Primary care validation of a single-question alcohol screening test. J Gen Intern Med 2009;24(7):783-88. [PMID: 19247718]
Smith P. C., Schmidt S. M., Allensworth-Davies D., et al. A single-question screening test for drug use in primary care. Arch Intern Med 2010;170(13):1155-60. [PMID: 20625025]
Solberg L. I., Maciosek M. V., Edwards N. M. Primary care intervention to reduce alcohol misuse ranking its health impact and cost effectiveness. Am J Prev Med 2008;34(2):143-52. [PMID: 18201645]
Sordo L., Barrio G., Bravo M. J., et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ 2017;357:j1550. [PMID: 28446428]
Spear S. E., Shedlin M., Gilberti B., et al. Feasibility and acceptability of an audio computer-assisted self-interview version of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in primary care patients. Subst Abus 2016;37(2):299-305. [PMID: 26158798]
Stade B. C., Bailey C., Dzendoletas D., et al. Psychological and/or educational interventions for reducing alcohol consumption in pregnant women and women planning pregnancy. Cochrane Database Syst Rev 2009;2009(2):CD004228. [PMID: 19370597]
Stewart S. H., Koch D. G., Willner I. R., et al. Validation of blood phosphatidylethanol as an alcohol consumption biomarker in patients with chronic liver disease. Alcohol Clin Exp Res 2014;38(6):1706-11. [PMID: 24848614]
Stringfellow, E. J.. Removing the X-waiver is one small step toward increasing treatment of opioid use disorder, but great leaps are needed. 2021 Apr 22. https://www.healthaffairs.org/content/forefront/removing-x-waiver-one-small-step-toward-increasing-treatment-opioid-use-disorder-but [accessed 2024 Mar 20]
Tori M. E., Larochelle M. R., Naimi T. S. Alcohol or benzodiazepine co-involvement with opioid overdose deaths in the United States, 1999-2017. JAMA Netw Open 2020;3(4):e202361. [PMID: 32271389]
Tourangeau R., Smith T. W. Asking sensitive questions: the impact of data collection mode, question format, and question context. Publ Opin Q 1996;60(2):275-304. http://www.jstor.org/stable/2749691
USPSTF. Final recommendation statement: tobacco smoking cessation in adults, including pregnant persons: interventions. 2021 Jan 19. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/tobacco-use-in-adults-and-pregnant-women-counseling-and-interventions [accessed 2024 Jan 16]
USPSTF(a). Final evidence summary: unhealthy drug use: screening. 2020 Jun 9. https://www.uspreventiveservicestaskforce.org/uspstf/document/final-evidence-summary/drug-use-illicit-screening [accessed 2024 Jan 16]
USPSTF(b). Final recommendation statement: unhealthy drug use: screening. 2020 Jun 9. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/drug-use-illicit-screening [accessed 2024 Jan 16]
USPSTF(c). Interventions for unhealthy drug use—supplemental report: a systematic review for the U.S. Preventive Services Task Force. 2020 Jun. https://www.ncbi.nlm.nih.gov/books/NBK558205/ [accessed 2020 Jan 7]
VA/DoD. Clinical practice guideline for the management of substance use disorders. 2015 Dec. https://www.healthquality.va.gov/guidelines/MH/sud/VADODSUDCPGRevised22216.pdf [accessed 2020 Mar 31]
Venkatesh V., Davis F. D. A theoretical extension of the technology acceptance model: four longitudinal field studies. Management Science 2000;46(2):186-204. http://www.jstor.org/stable/2634758
Verstraete A. G. Detection times of drugs of abuse in blood, urine, and oral fluid. Ther Drug Monit 2004;26(2):200-205. [PMID: 15228165]
Wakeman S. E., Larochelle M. R., Ameli O., et al. Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Netw Open 2020;3(2):e1920622. [PMID: 32022884]
Wang L., Min J. E., Krebs E., et al. Polydrug use and its association with drug treatment outcomes among primary heroin, methamphetamine, and cocaine users. Int J Drug Policy 2017;49:32-40. [PMID: 28888099]
Wartko P. D., Bobb J. F., Boudreau D. M., et al. Nurse care management for opioid use disorder treatment: the PROUD cluster randomized clinical trial. JAMA Intern Med 2023;183(12):1343-54. [PMID: 37902748]
Watts B. V., Gottlieb D. J., Riblet N. B., et al. Association of medication treatment for opioid use disorder with suicide mortality. Am J Psychiatry 2022;179(4):298-304. [PMID: 35360916]
White A. M., Castle I. P., Hingson R. W., et al. Using death certificates to explore changes in alcohol-related mortality in the United States, 1999 to 2017. Alcohol Clin Exp Res 2020;44(1):178-87. [PMID: 31912524]
WHO. The health and social effects of nonmedical cannabis use. 2016 Nov 11. https://www.who.int/publications/i/item/9789241510240 [accessed 2020 Mar 31]
Wight R. G., Rotheram-Borus M. J., Klosinski L., et al. Screening for transmission behaviors among HIV-infected adults. AIDS Educ Prev 2000;12(5):431-41. [PMID: 11063062]
Williams E. C., Achtmeyer C. E., Thomas R. M., et al. Factors underlying quality problems with alcohol screening prompted by a clinical reminder in primary care: a multi-site qualitative study. J Gen Intern Med 2015;30(8):1125-32. [PMID: 25731916]
Yudko E., Lozhkina O., Fouts A. A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. J Subst Abuse Treat 2007;32(2):189-98. [PMID: 17306727]
Zarse E. M., Neff M. R., Yoder R., et al. The adverse childhood experiences questionnaire: two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Medicine 2019;6(1):1581447. https://doi.org/10.1080/2331205X.2019.1581447
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | October 21, 2020 |
| Date of current publication | May 30, 2024 |
| Highlights of changes, additions, and updates in the May 30, 2024 edition |
|
| Intended users | Primary care clinicians and care providers in other adult outpatient care settings in New York State |
| Lead author(s) |
Jennifer McNeely, MD, MS; Leah K. Hamilton, PhD; Susan D. Whitley, MD |
| Writing group |
Timothy J. Wiegand, MD, FACMT, FAACT, DFASAM; Sharon L. Stancliff, MD; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD; Christopher J. Hoffman, MD, MPH, MSc, FACP |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
Guidelines
GuidancePodcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on March 27, 2026